 The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.
The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.It was written in german and was translated into more than 10 languages already. German is not freely available, as the rights are held by a publisher, but all these translations are available as ebooks / PDFs for free, as a gift of Björn for you, for the New Earth, for a new time.
In cooperation with Björn, it is splitted on "Disease is Different" into the sections by organ systems and combined with the real cases of our international testimonial / report archive of the related organ system.
BREAST
The female breast is, in principle, a protrusion of the skin over the pectoral muscles. Old-mesodermal mammary glands are found embedded in fatty tissue. These evolved from the sweat glands over the course of our developmental history.
The milk (lactiferous) ducts are lined with ectodermal epithelium, which migrated from the outer skin. They guide milk from the lobe of the breast to the nipple.
Epidermis, Nipples
Separation conflict
Dermis
Disfigurement
conflict
Mammary Gland
Excretory Ducts
Separation conflict

Mammary Glands
Worry, fight or
nest conflict
Lymph Nodes
Self-esteem conflict
Breast cancer (mammary carcinoma, inflammatory breast cancer = IBC)
There are two different types of breast cancer. The name “breast cancer“ says nothing about which type is meant. About 80% of the time, the milk ducts are affected; in the other 20% the mammary glands are.

Cancer of the mammary glands (adeno-ca, lobular
breast cancer, lobular carcinoma in situ = LCIS)1
| Conflict | Right-handed woman, left breast: worry or fight conflict with regard to the mother-child or “nest“; right breast: worry or fight conflict with regard to the partner. Left-handed woman: inverse. Further possibilities: Conflict in relation to being able to feed, give, be there for someone. Nest conflict: The home is in danger, one fears for one‘s house or apartment, fighting in or about the house or apartment. |
|---|---|
| Examples |  A 43-year-old, left-handed woman is blamed by her daughter for having destroyed her marriage = mother-child fight conflict. A tumor of the right breast develops. (Archive B. Eybl) A right-handed woman embarks on a week-long vacation with friends, while her ex-husband cares for their epileptic daughter. On the very first day of the vacation, she receives a phone call from home: her ex-husband reports that their daughter has had a severe epileptic fit and is currently in the hospital. He blames his ex-wife (the patient) for not being there. She wants to fly back to her daughter right away but is unable to book a flight = mother-child worry conflict – one week of very strong conflict activity. A breast-gland tumor develops in the left breast. In the following years, the patient remains mildly conflict-active because she is expecting another fit at any time. Not until the daughter has been stable for several years does she come into healing: the patient sweats at night, the breast reddens, swells up and after six weeks breaks open and gives off stinking pus. (Archive B. Eybl) A woman moves to a large city in a colder climate for her education where she has to accept living in a dark, inner-courtyard apartment. Accustomed to a sunny climate, she is unhappy in the apartment and longs for life-giving sunlight. She comes to the conclusion that “everything is so dark in this land“ = nest conflict. To relieve her distress, she moves her bed right up to the window so she can “catch” a little light. Subsequently, she is diagnosed with breast gland cancer. (Archive Antje Scherret) A 44-year-old has a pubescent daughter who is driving her crazy. They are constantly arguing – it has even gotten to the point where they avoid each other = mother-child fight conflict. A tumor develops in a breast gland. As their relationship suddenly improves, the tumor comes into healing. (Archive B. Eybl) A 65-year-old, right-handed patient takes care of her granddaughter during the day. One summer day, she holds a children‘s party in the garden and the patient‘s dog joins in. In their excitement, the children come up with the idea of riding the dog. The dog does not like the idea and bites one of the children. The wound is not serious, but at the hospital, charges are brought against the dog‘s owner. The patient is afraid that she will have to give up her beloved dog = mother-child worry conflict involving a dog. A breast gland tumor develops. When the charges are dropped, she comes into healing and is diagnosed with a mammary gland cancer. (Archive B. Eybl) A 43-year-old, left-handed woman is blamed by her daughter for having destroyed her marriage = mother-child fight conflict. A tumor of the right breast develops. (Archive B. Eybl) A right-handed woman embarks on a week-long vacation with friends, while her ex-husband cares for their epileptic daughter. On the very first day of the vacation, she receives a phone call from home: her ex-husband reports that their daughter has had a severe epileptic fit and is currently in the hospital. He blames his ex-wife (the patient) for not being there. She wants to fly back to her daughter right away but is unable to book a flight = mother-child worry conflict – one week of very strong conflict activity. A breast-gland tumor develops in the left breast. In the following years, the patient remains mildly conflict-active because she is expecting another fit at any time. Not until the daughter has been stable for several years does she come into healing: the patient sweats at night, the breast reddens, swells up and after six weeks breaks open and gives off stinking pus. (Archive B. Eybl) A woman moves to a large city in a colder climate for her education where she has to accept living in a dark, inner-courtyard apartment. Accustomed to a sunny climate, she is unhappy in the apartment and longs for life-giving sunlight. She comes to the conclusion that “everything is so dark in this land“ = nest conflict. To relieve her distress, she moves her bed right up to the window so she can “catch” a little light. Subsequently, she is diagnosed with breast gland cancer. (Archive Antje Scherret) A 44-year-old has a pubescent daughter who is driving her crazy. They are constantly arguing – it has even gotten to the point where they avoid each other = mother-child fight conflict. A tumor develops in a breast gland. As their relationship suddenly improves, the tumor comes into healing. (Archive B. Eybl) A 65-year-old, right-handed patient takes care of her granddaughter during the day. One summer day, she holds a children‘s party in the garden and the patient‘s dog joins in. In their excitement, the children come up with the idea of riding the dog. The dog does not like the idea and bites one of the children. The wound is not serious, but at the hospital, charges are brought against the dog‘s owner. The patient is afraid that she will have to give up her beloved dog = mother-child worry conflict involving a dog. A breast gland tumor develops. When the charges are dropped, she comes into healing and is diagnosed with a mammary gland cancer. (Archive B. Eybl) |
| Conflict-active | Cell division in the mammary gland tissue, growth of one or more nodes (= adeno-ca); the longer and more intense the conflict is, the larger the tumor grows. If a tissue sample is taken during the growth, medicinal practitioners will speak of “malignant cancer.“ If one does not find an above average rate of cell division (= resolved conflict) under the microscope, the diagnosis may be “benign.“ In the conflict active phase, there is a tendency to be over-caring/over-protective and to “hover.” Often a recurring–conflict. |
| Bio. function | With more mammary gland tissue, more milk can be produced. With the extra food supply, the child or family member can heal faster. One can feed and give more. |
| Repair phase | Caseating, tubercular degradation if bacteria are present; the cell remnants are eliminated over the lymph system. Although the tumor is no longer growing, the breast swells up at the beginning of the repair phase because of the increased metabolism. Pain, night sweats, possibly slight fever; only later in the process do the nodes and breast feel smaller. Especially strong swelling caused by syndrome > danger of panic, if no bacteria are available, the tumor will be encapsulated and separated from the body‘s metabolism (CM: “benign“); the tumor remains but is no longer malignant. |
| Repair crisis | Chills or a feeling of being cold, severe pain. |
| Note | The tumor can break open externally if, due to the tumor or puncture, the woman has also suffered a disfigurement conflict affecting the dermis or in the case of a superficially located tumor, the skin no longer can hold up to the pressure > bloody, oozing, stinking, degradation of the tumor outwardly (= open breast tuberculosis). An external eruption may cause a vicious conflict circle. Consider “handedness“ (right or left) and side (mother/child or partner) or local conflict. |
| Questions | First, determine if the mammary glands or lactiferous ducts are affected. (Medical history, touch and visual findings, x-ray, CT, biopsy). Study the findings, but keep in mind that CM often misses the mark. (Absurd diagnoses like “ductal-adenoidal mammary carcinoma” are not so rare). Was/is the nipple drawn-in? (Yes > sure indication for lactiferous ducts. No > indication for mammary glands). “Micro calcifications” in the findings? (Indication of lactiferous ducts). The nearer the nodes are to the nipple, the more likely that it is the lactiferous ducts. Reddening of the skin or nipple? (Yes > indication for lactiferous ducts) Are the nodes painful/hot/reddened? (Yes > indication of the repair phase of both SBSs). When was the last examination? (Good possibility that the conflict is located within this time frame). Open ulcerations on the breast? (Yes > persistent conflict, both SBSs come into question). Nodes tangible since when? (Conflict considerably earlier – take the development time into account). General sign of conflict activity during the growth of the node(s)? (Waking up early in the morning, poor sleep, weight loss, stress, no night sweats)? Yes > indication for mammary glands. General repair phase signs during the node-growth phase? (Good sleep, cheerful emotionally, good appetite, light night sweats? Yes > Indication for lactiferous ducts). If we now know that we are dealing with an SBS of the mammary glands, perform the clap test. Which worry, fight or nest conflict was there? Who was I unable to feed anymore? What stressed me? What was I constantly thinking about? Why can’t I deal with the issue? What has conditioned me? Did ancestors suffer from breast cancer? (Yes > work out any similar character traits/family issues). Which beliefs fed the conflict? (Beliefs that kept me from dealing with/resolving the conflict = disease-causing beliefs)? Would a conversation/discussion to clarify the issue be helpful? (E.g., with the person the conflict is centered around)? Which new inner attitudes would ease my mind? What can I change on the outside? |
| Therapy | Determine the conflict and conditioning and, if possible, resolve them in real life should they still be active. Guiding principles: “Don‘t worry, live!“ “My worries won‘t help anyone!“ “I am not responsible for everyone. Destiny knows what’s best.“ “Life is too precious to spend it bickering over trifles.“ Surgery – yes or no? If the tumor is too large, it is doubtful whether the patient will be able to survive a long-lasting breast-tuberculosis. For this reason, surgery is recommended. The doctor should use care, to only remove the tumor, leaving the lymph nodes in place. Caution: After the OP (disfigurement of the breast), the patient often suffers from a self-esteem conflict in the repair phase. > Growth of breast-lymph nodes > danger of a vicious circle if an understanding of the correlations is lacking. Here too, surgery may be advisable. If applicable, instead of surgery, black salve is an option for people who have a high tolerance for pain and very strong nerves (order at www.cernamast.eu). CM: chemotherapy and anti-hormone therapy (anti-estrogen or aromatase inhibitors) are not recommended, because of adverse side effects. See also: remedies for the breast on p. 331. |
Adhesions on the breast glands (sclerosing adenosis, fibroadenoma)
Same SBS as above.
| Phase | Condition following the repair phase or following reoccurrences = scarred remnant of a healed breast gland tumor. |
|---|---|
| Therapy | The conflict is resolved. If the breast continues to change, this means that the conflict has not been conclusively resolved. > Need for therapy: questions, conflict resolution (see above), OP as necessary. Gentle massages or lymph drainage massages (see p. 68) with marigold salve, so that the tissue becomes smooth and supple again. Daily morning ritual by Anton Styger (see: p.83). |
11 See Dr. Hamer, Charts pp. 45 ff, 50 ff

Intraductal cancer (ductal carcinoma in situ = DCIS, lobular cancer in situ = LCIS, invasive lobular cancer, ductal hyperplasia, papillary adenoma, Paget‘s disease)1
| Conflict | 1. Right-handed woman, left breast: separation conflict related to mother/child; right breast: separation conflict related to partner. Left-handed woman: inverse, i.e., conflicts are reversed. Mother/child or partner has pulled away from the breast. 2. One feels “sucked dry.” Mother/child or partner is too demanding – one’s own energies are dwindling. One can’t go on anymore. Note: This conflict possibility corresponds with the separation conflict of undesired skin contact (wanting to be separated from someone). |
|---|---|
| Examples | ➜ A woman‘s daughter moves to a city far away. ➜ A woman finds out that her partner is unfaithful. A left-handed, happily–married woman has a son, whom she loves above all else. At the beginning of his studies, he is still living at home with his parents. She is severely affected by his announcement that he plans to move into his own apartment. She never imagined that he would leave so quickly. For her, he was always her “little boy“= conflict that her son is being pulled away from her breast > unnoticed cell degradation in the lactiferous ducts in the active-phase. One day, after the patient has accepted that her son‘s leaving is a positive and normal development, she notices a lump in her right mother-child breast. CM: invasive ductal carcinoma. (See Claudio Trupiano, thanks to Dr. Hamer, p. 298) A 39-year-old, right-handed patient has a number of fierce disagreements with her husband about his ex-wife. In her opinion, he is too friendly and cooperative toward her = partner-separation conflict affecting the lactiferous ducts of the right breast > cell degradation in the active-phase, restoration (= intraductal cancer) in the repair phase. (Archive B. Eybl) A 41-year-old, childless, right-handed patient has a dog named Benni whom she loves very much. She makes it clear to her mother, who lives on a farm, that she mustn‘t lay out any rat poison because that could endanger Benni. Her mother ignores her warnings and misfortune strikes: Benni eats the poison and dies. Her pet-child is “pulled away from the breast.” She doesn‘t want to talk about it to anyone, because Benni was “just a dog“ > cell degradation in the active–phase. Not until a year later, does the patient recover from the incident. In the repair phase, she notices a white lesion on the left nipple. A 2x2x4 cm lump develops in the lactiferous ducts. The patient is relieved as she learns about the causal relationships and refuses CM-treatment. Within a year, the lump is almost gone. (Archive B. Eybl) A 42-year-old, right-handed married patient, mother of two children, has a husband who is very much under his mother‘s influence. The patient‘s mother-in-law tries to pull the two children onto her side and this has nearly ruined their marriage. On Christmas, her husband takes the children “for a quick visit“ to his parents. However, he and the children stay and celebrate with the mother-in-law = mother-child separation conflict – the children are “torn from her breast.” (Archive B. Eybl) An example of a less frequent conflict possibility resulting from unwanted skin contact: A sensitive, right-handed woman has a naturally low energy level. Her pubescent son makes incessant demands on her, even though she already gives him everything. She also doesn’t feel supported by her partner = separation conflict – she feels like the life is being sucked out of her. She is diagnosed with a mammary gland carcinoma on the mother/child side. (Archive B. Eybl) |
| Conflict-active | Limited sensibility = numbness (usually unnoticed). Simultaneous slackening of the lactiferous duct’s ring musculature. Later, epithelial cell degradation in the lactiferous ducts (ulcer) > increase in lumen. With longer conflict activity, the lactiferous ducts shrink up painfully. The nipple or the affected spot is pulled inwards (so-called “inverted nipple,“ CM: cirrhotic lactiferous duct ulcer). After longer conflict activity and if many lactiferous ducts are affected, the breast can become smaller as a whole. Possibly a recurring conflict. |
| Bio. function | 1. Through the numbness, the separation is easier to forget. It no longer feels so strong. 2. Expansion of the lactiferous ducts, so that the milk does not become blocked and can drip out by itself, because, due to the separation, the child or family member cannot drink the milk. |
| Repair phase | Restoration of the epithelial mucosa (= CM: “intraductal mammary cancer,“ periductal mastitis), swelling, itching, pain. In this SBS, the outer skin often reacts with a reddening of the breast in the repair phase. Secretions (bloody or clear) build up in the milk ducts due to increased metabolism. However, since the milk ducts are swollen closed, the fluid can back up behind the nipple, especially with an active kidney collecting tubules SBS = syndrome. After the completion of the repair phase, the breast shrinks, dimpling and hardenings and (micro) calcifications possibly remain. The nipple usually stays inverted. |
| Repair crisis | Feeling cold, possibly chills, and severe pain. Possibly blood/secretions leaking from the nipple. |
| Note | Cancer of the nipple is called “Paget‘s disease“ in CM. Tissue-wise, they belong to the lactiferous ducts = same SBS. Consider “handedness“ (right or left) and side (mother/child or partner) or local conflict. |
| Questions | Determine which breast SBS (see also questions on p. 326) . Nipple inverted? (Yes > indication of an extended active conflict). Nodes since when? (= Start of the repair phase or the start of a chronic process). Has the breast changed unpleasantly? (= Indication of a recurring conflict). Clap test/handedness? Who was torn from my breast or from whom do I feel “sucked dry?” (E.g., by my child, partner)? Why do I react so sensitively? Who/what has conditioned me when it comes to separation/distance? (E.g., parents’ divorce, death of a sibling)? How was my birth? Was I with my mother? Was I a planned child? Am I similar to one of my parents? (Work out family issue(s)). Breast cancer in the family? Which mediation/which guiding principle would be helpful? What else do I want to change inside? What outside? |
| Therapy | The conflict is resolved. Support the healing process. Determine the conflict and conditioning if still active. Guiding principles: “I love you, and that is why I am letting you go.“ “I am setting you free.“ For a blockage: Somebody (partner, child) should suck out the secretion orally, like a baby. Surgery if the tumor becomes too large due to recurrences. Remove only small areas (not too far into the healthy tissue). Caution: The surgery is often followed by a breast self-esteem conflict in healing > growth of breast-lymph nodes > danger of a vicious circle, if the interrelationships are not understood. Anti-hormone therapy (anti-estrogen or aromatase inhibitors) is not recommended because of the numerous side effects. See also: remedies for the breast on p. 331. |
Small calcifications in the breast (micro calcifications)
Same SBS as above. Calcifications, often only pin-sized, are sometimes found in the mammography and are seen as possible “signs of cancer.“ Calcifications also remain after breast gland tuberculosis.
| Phase | Condition after the repair phase. Completed and finished or recurring lactiferous ducts SBS. In principle, after the healing swelling or scarring in the lactiferous ducts, this is “left-over,” calcified milk. |
|---|---|
| Therapy | The conflict is resolved. No further measures needed, except – prevent recurrences! |
1 See Dr. Hamer, Charts pp. 120, 133
Melanoma on the breast
| Conflict | Disfigurement conflict: the feeling that the breast is disfigured, violation of integrity. |
|---|---|
| Examples | A breast cancer patient feels disfigured because of the tumor in her breast. A widespread melanoma develops. Note: very common follow-up conflict, interpreted by CM, as “metastases“ > danger of a vicious circle. (Archive B. Eybl) A woman has recently weaned her third child from the breast. One day, as she is sitting alone in bed, she notices her limp, drooping bosom and has feelings of anxiety = disfigurement conflict with regard to the dermis. At the spot she finds especially unattractive, she develops a 5 mm melanoma = growth in the conflict-active state. (Archive B. Eybl) |
| Conflict-active | Cell division in the dermis, growth of a melanoma = common follow-up conflict to breast cancer. |
| Bio. function | Strengthening as protection from disfigurements or damages to integrity. |
| Repair phase | Caseating degradation via bacteria (mycobacteria), or bacteria. |
| Questions | In the case of small melanomas, one sometimes doesn’t find the cause (minimal limit). Since when has it been growing? (Conflict time frame). Is it bleeding while degrading? (No > indication of an active conflict). By what do I feel attacked/injured? (Breast cancer, real blow, groped, harmful words)? Is this why I’m upset? (Yes > OP). Which new attitude would be helpful? (E.g., to develop a healthy robustness)? |
| Therapy | Determine the conflict and conditioning and, if possible, resolve them in real life if still active. Doing nothing is possible with small melanomas when the patient has no fear whatsoever. If the patient thinks about it constantly, one should have it removed for the purpose of minimizing risk. If necessary, black salve or surgery (see pp. 341, 351). |
Vasospasm of the arterioles (Raynaud’s phenomenon of the nipple)
Symptoms: Severe, pulling-stabbing pains in the nipple, most often in breast-feeding mothers, but also often continuing after breast-feeding has ended.
The nipple is pale/blue and sensitive to cold.
Most of the affected also suffer from Raynaud symptoms somewhere else on their body (see: p.174).
At the beginning of the illness, the symptoms are often difficult to differentiate from a nipple inflammation (thelitis, mastitis).
| Conflict | Not wanting to come in contact with/get close to death or a dead body. The situation must have a connection to conception, pregnancy, nursing, offspring or the family. |
|---|---|
| Example | The breast-feeding mother suffers from Raynaud’s phenomenon of the nipples. During the pregnancy, a close relative died, but the young woman didn’t want to hear anything about it. She repressed the death itself and didn’t go to the funeral. Conflict that she doesn’t want to come into contact with the death. (Archive B. Eybl) |
| Phase | Persistent active conflict. Tension in the vascular musculature > insufficient oxygen supply to the nipple > white discoloration, pain during sympathicotonia. |
| Questions | When did the symptoms begin? Experience with dead people/animals during or before the pregnancy? How did I deal with it? Are there repressed corpse experiences among the ancestors? (Ask the parents, look for conditioning). Beliefs with regard to death/dying? (E.g., “death is something dreadful”). |
| Therapy | Determine and resolve the conflict, beliefs and conditioning. Heat treatments (hot showers/baths, hot water bottles, warm wraps). Guiding principle: “I acknowledge what was and I make my peace with it completely.” Healing conversation. Farewell ritual. Come to terms with death. See also: remedies for the breast on p. 331. |
Inflammation of the breast glands (mastitis), inflammation of the nipple (thelitis)
Both SBSs come into question. The condition usually appears during the postpartum period (mastitis puerperalis).
Both inflammation of the mammary glands, as well as inflammation of the nipples or milk ducts, are called mastitis by CM.
| Example | ➜ The baby is born healthy and is nursing well. The worries of pregnancy have all been forgotten = beginning of the repair phase > inflamed breast gland or nipple. |
|---|---|
| Phase | Repair phase of both SBSs in question. |
| Note | An inflamed nipple can also have a mechanical cause, e.g., if the infant sucks too vigorously. |
| Therapy | The conflict is resolved. Support the healing. Avoid recurrences. Apply quark (curds) or healing clay. Colloidal silver, MMS or CDL (see p. 68) internally and externally. See remedies for the breast p. 331. |
Shape changes of the breast
Lumps
- Milk glands in the active–phase or repair phase.
- Excretory ducts in the repair phase.
- Active kidney collecting tubules SBS (see: p.277) can cause old lumps to be “pumped up“ again, giving the false impression that a new SBS of the breast is underway.
Skin indentations or inverted nipples
- Mammary ducts in active-conflict or following recurrences (see: p.327).
- In women with generally weak connective tissue, the breasts drop in early years, because the collagenous fibers are soon thinned out = indication of reduced self-confidence (mild general self-esteem conflict). Usually the low self-esteem and “weak connective tissue“ is passed down over several generations. See: p.346)
- In women with normal to good connective tissue, sagging breasts can come from an SBS of the lactiferous ducts, if previously full lumps collapse after dissolving (see: p.327).
- If a woman has firm breasts due to an active refugee conflict, the breasts will collapse after the resolution of the conflict > Good sign! Indicated by fluid loss, weight loss, night sweats (see: p.277).
- Active kidney collecting tubules SBS (see: p.277) can provide attractively firm breasts. Disadvantages: This is usually accompanied by becoming overweight, edema, and fat deposits due to a refugee conflict. If the conflict is resolved, the breasts usually shrink and appear relatively less attractive.
- Bach flowers (see p. 59): red chestnut, chicory, willow.
- Teas: tea or tea compresses: marigold, yarrow, fennel, chamomile, comfrey, yellow meliot.
- Schuessler Cell Salts: No. 3, 11, 12.
- Enzyme preparations for inflamed breasts.
- Lymph drainage massages (see p. 68), gentle massages.
- For an open wound on the breast: Apply honey, change wound compresses regularly.
- Beat curly-leaf cabbage and white cabbage until soft and apply regularly.
- A silver activated charcoal bandage is useful against the unpleasant odors of tuberculosis.
- MMS (see p. 68).
- Hydrogen peroxide (H2O2) internally and externally.
All experience reports on the organ system „Breast” from the International Report Archive:
| Author | Title and Overview | Keywords | ||||
|---|---|---|---|---|---|---|
 | 2026/03/01   My wife died of lung cancer at the age of 35, leaving me (38) and our six children behind. Four years later, I would like to tell you what happened to me after my wife's death: About 6-7 weeks after her death, I noticed a bean-sized lump under my left nipple. It grew slightly larger over the following days... | |||||
 | 2025/10/23 In January 2024, during a routine mammogram, Marta present a 4mm X 3mm nodule is detected; the diagnosis: Ductal Carcinoma. There are no symptoms, it is possibly a cold nodule from a previous episode. In June 2024, there is a new 28mm x 20mm nodule and there are symptoms: itching, burning, inflammation and local heat; the diagnosis: Right breast carcinoma In October 2024, the nodule has been reduced by half, now 14mm. Marta has experienced a new separation conflict with her mother that has now been resolved and she has found and applied a strategy to avoid entering into a separation conflict with her mother again.  | Separation conflict, ductal carcinoma | ||||
 | 2025/09/24 Several events, only on the supposedly “wrong” side - we found a clear page shift | Perceiving one's partner as a child | ||||
| 2025/08/17 A 53-year-old right-handed woman, the diagnosis (May 2024) was: Ductal carcinoma of the right breast, Birad 5-6, size 1.6 cm. | Separation conflict, ductal carcinoma | ||||
| 2025/08/17 A ductal carcinoma of the right breast caused by a biological conflict related to the partner of a right-handed woman. | Separation conflict, ductal carcinoma | ||||
| 2025/08/15 Breast Cancer right side due to "contact guilt" during the coronavirus pandemic. Brilliant and precise timing. | Breast cancer right side | ||||
 | 2025/06/12 I had an unexpected separation around a relationship that felt “ripped away” from my breast in February of 2024. It was very distressing to me and lasted for 4 months. In May of 2024, I noticed, whilst drying off from a shower, that my right nipple appeared to be retracting ... | Breast cancer | ||||
| 2025/06/12 It all started in 2016 when I was diagnosed with ER positive, HER2 negative, left breast ductal cancer which was tackled with some deep breaths, a lumpectomy and holistic healing ... | |||||
| 2025/06/12 In May of 2022, while 31 weeks pregnant, I was diagnosed with triple-positive breast cancer (ductal). Almost immediately, I underwent a lumpectomy and sentinel node biopsy at 33 weeks pregnant and was then induced at 37 weeks to be able to recover for a month before starting chemotherapy in August ... | |||||
| 2025/06/12 In ten days, I'd gone from a happy, carefree 46-year-old to a “diseased” breast cancer patient who was being strongly advised to have a mastectomy, radiation on my breast wall, and then follow a course of life-limiting drugs to both prolong and, indeed, save my life. I didn't even have any symptoms ... | |||||
| 2025/06/12 I noticed a painful lump in my right breast, near the nipple. I’m right-handed. Soon after, two more lumps followed, one at about 3:00 and the other at 6:00 o’clock in the breast. I wondered what this was about? ... | breast cancer | ||||
| 2025/06/10 My experience started on the 28th of January 2022, at the age of 75 years old. I found a lump in my left breast. That date is also my two sons’ birthdays, both born on the same day four years apart. At the time, I was not too concerned but asked my guardian spirits to help me find the right treatment ... | |||||
| 2025/06/10 The three scariest words you could hear in the English language are “you have cancer.” No other phrase will take the wind out of your sails and instill such fear as this powerful phrase. Personally, I have heard these words, not once, not twice, but three times… with each diagnosis a more serious, sinister, and terrifying one. | |||||
2025/03/24 This documentary presents 15 individuals who were diagnosed with cancer by conventional medicine and who examined the causes of their symptoms according to the model of the so-called 5 Biological Laws of Nature and overcame them.  | Colon cancer, bone cancer, breast cancer, skin cancer, testicular cancer, pancreatic cancer, cervical cancer | |||||
 | 2025/03/10 At the beginning of May 2024, I noticed a small round lump in my left breast. It was not visible externally, and nothing else had changed externally. But when I touched it, the area was sensitive. I would say it felt inflamed under the skin...  | Breast cancer | ||||
 | 2025/03/05 A mother of four children came to us with a diagnosis of breast cancer and wanted to know what Germanic Medicine had to say about it in parallel with her medical treatment. After working together for three months, the two small tumors (5 mm and 8 mm) that had previously been diagnosed were no longer visible. In summary, I have found that close, intensive cooperation over a relatively short period of time is a good method for resolving even complex illnesses. Focusing all your attention on your own body for a long time can really make a difference. | Nest worry and care conflict | ||||
2025/02/14 Yaara Kaizer from Israel was diagnosed with ductal breast cancer, i.e. affecting the ectodermal milk ducts, in 2017 ... 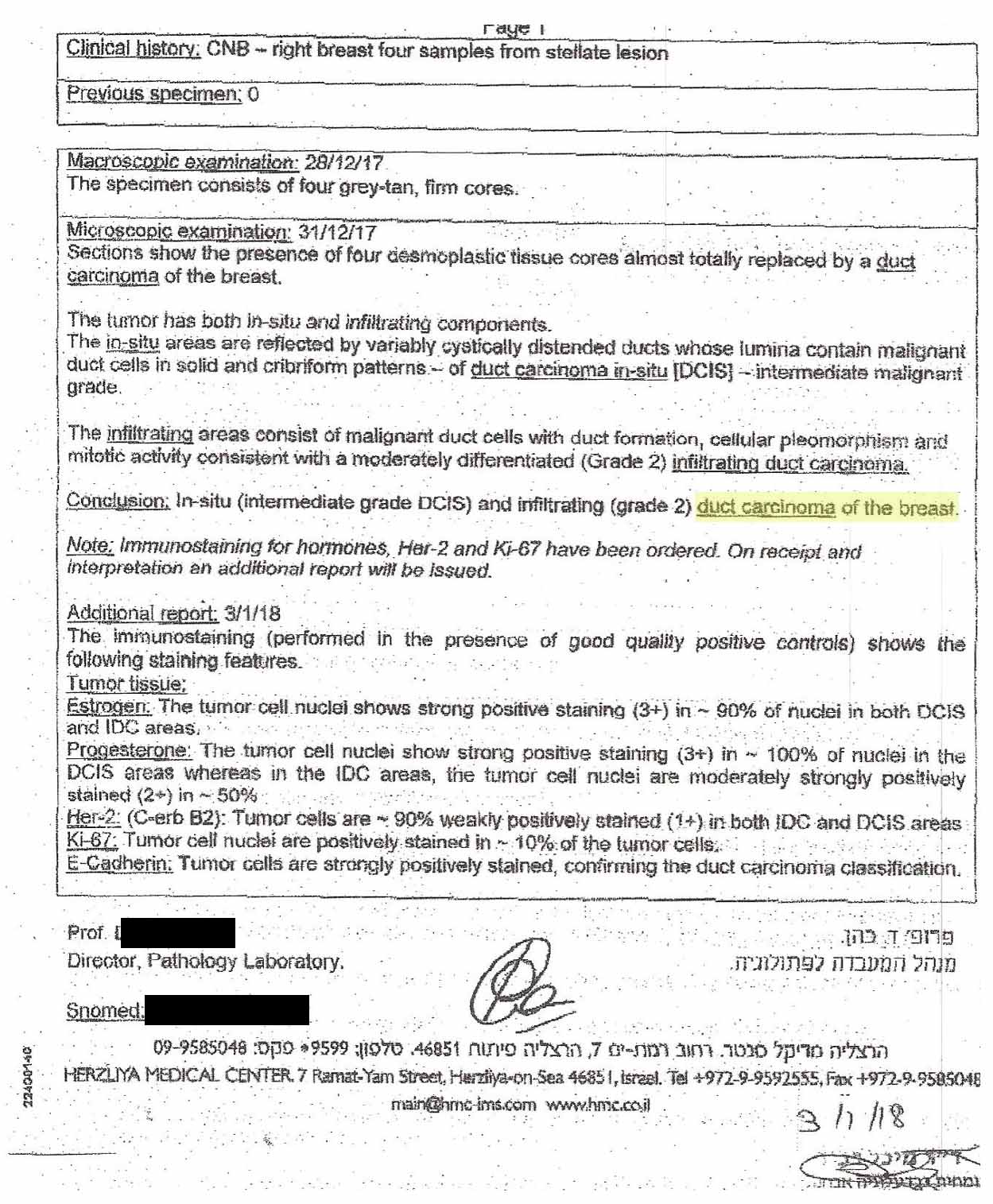 | ||||||
2025/02/11 I felt a lump in my left breast and two in my right breast in the shower in the evening in December 2023. For the 4 weeks before that, my breasts had always been quite swollen, they hurt and I can remember that I was already experiencing night sweats at night in November. 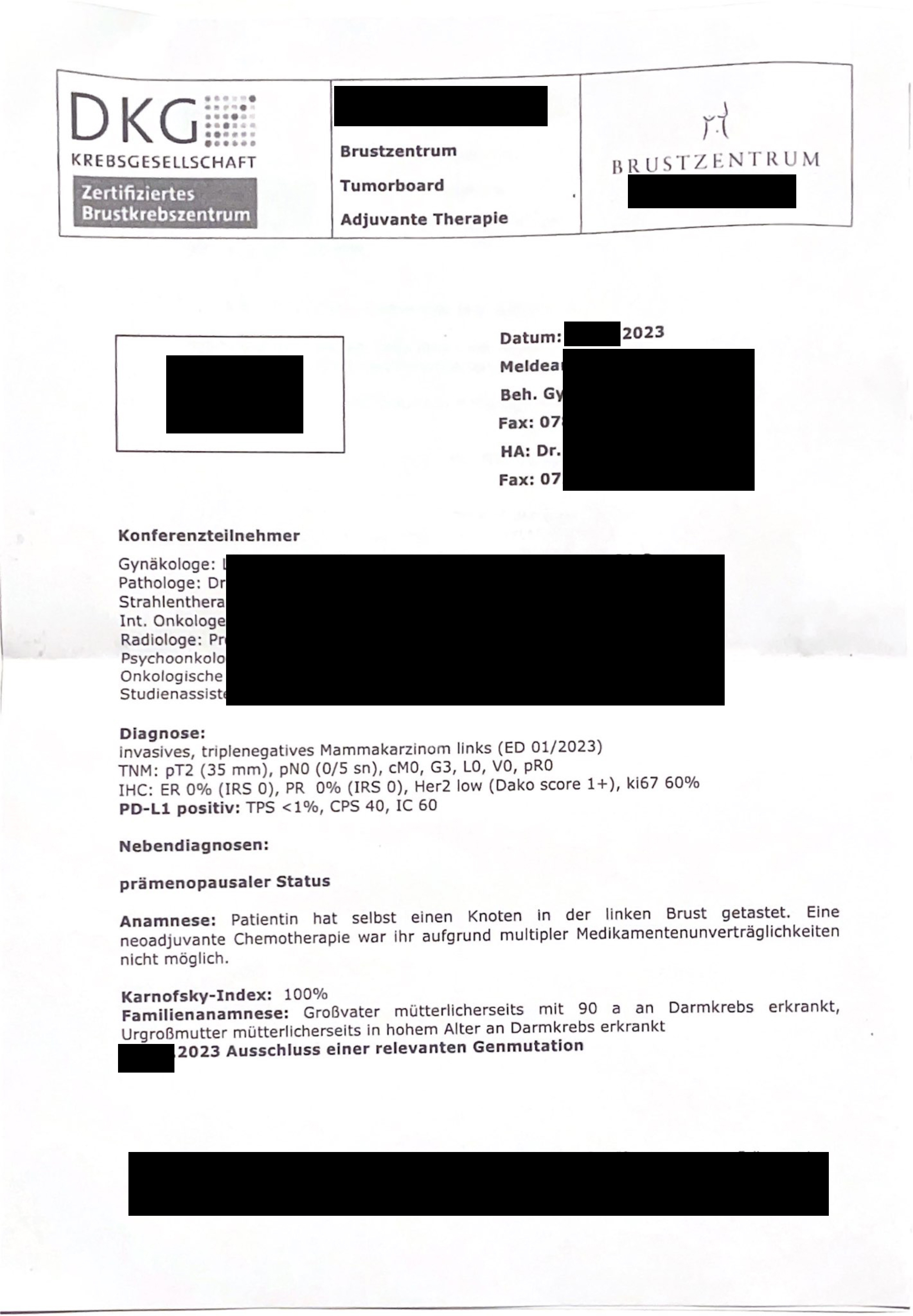 | Breast cancer | |||||
| 2024/01/24 I have been living separately from my ex-husband for 6 years. My children are alternately with him or with me. It happened that my ex-husband called me on his way home from work and said that my daughter had fallen down the stairs at his house. As my daughter had fallen unconscious, his girlfriend, who lives with him, had called an ambulance. She would now take her to hospital ... | |||||
 | 2022/09/15   A woman with a breast cancer in the left breast  | Breast Cancer | ||||
 | 2021/03/12 A woman 40 year old came to me with a medically diagnosed case of breast cancer. She had 2 adenocarcinomas and one intraductal tumor. These tumors ranged in size from 3 to 5 cm. The medical doctors wanted to perform a mastectomy's and then subject her to chemotherapy. After the understanding of the cause and our therapy, she was declared cancer free by her oncologist 4 months later. No chemo, no drugs or scalpel. The oncologist didn't know what to say. | |||||
| 2021/03/12 In these report are different symptoms combined, as they nearly all were the deleterious results of 20 years of being married to a covert narcissist. After a second, very happy marriage, I developed symptoms of "breast cancer" after the sudden death of my wife. | |||||
| 2019/09/02 A few months after her husband's funeral, she was diagnosed with breast cancer in her right breast and treated with conventional medicine. The affected tissue (without histological findings) must have been the ectodermal milk ducts, i.e. the content of the conflict: “My partner was torn from my breast.” | Torn from chest, milk ducts | ||||
| 2015/01/01 Here is a list of other sources where experience reports with the 5BN can be found, e.g. to:: Bursitis, conjunctivitis, rheumatism, diabetes, hay fever, psoriasis, bedwetting, stuttering, oceans, aggressive constellation, endometrial CA, cervical cancer, shingles, tinnitus, toothache, heart attack, high blood pressure, colic, slipped disc, knee pain, leukemia, bone cancer, voice gone, stomach pain, hives, Epilepsy, intolerances, Crohn's disease, skin rash, facial paralysis, hiccups, anorexia, bronchitis, corneal inflammation, migraine, thyroid cyst, aphthae, osteolysis, gastritis, rectal spasms, milk duct carcinoma, allergies, hepatic coma, gray hair, nail fungus, heartburn, nasal polyps, caries, heart attack, ankylosing spondylitis, melanoma, psoriasis, water belly, hailstones, prostate, . .. |